If you’re losing your teeth in your 40s or 50s, you’re not alone. I see many patients around this age who have lost several, or even all, of their teeth. Today I want to share the story of one of my patients — a wonderful man in his late 40s — who decided it was time to get his life and smile back.
This case walks through his transformation with full upper replacement (All-on-6) and a lower implant bridge, combined with deep cleanings to save the rest of his healthy teeth.
When Life Catches Up
In our 20s and 30s, we feel invincible. Then one day, in our 40s or 50s, we realize time and health issues have caught up with us. Over the years, I’ve treated thousands of patients in this age range who needed full mouth extractions and full dental implants or are just losing several teeth.
Life gets busy. Dental care often takes a back seat. But the good news is, it’s never too late to fix it.
The First Visit
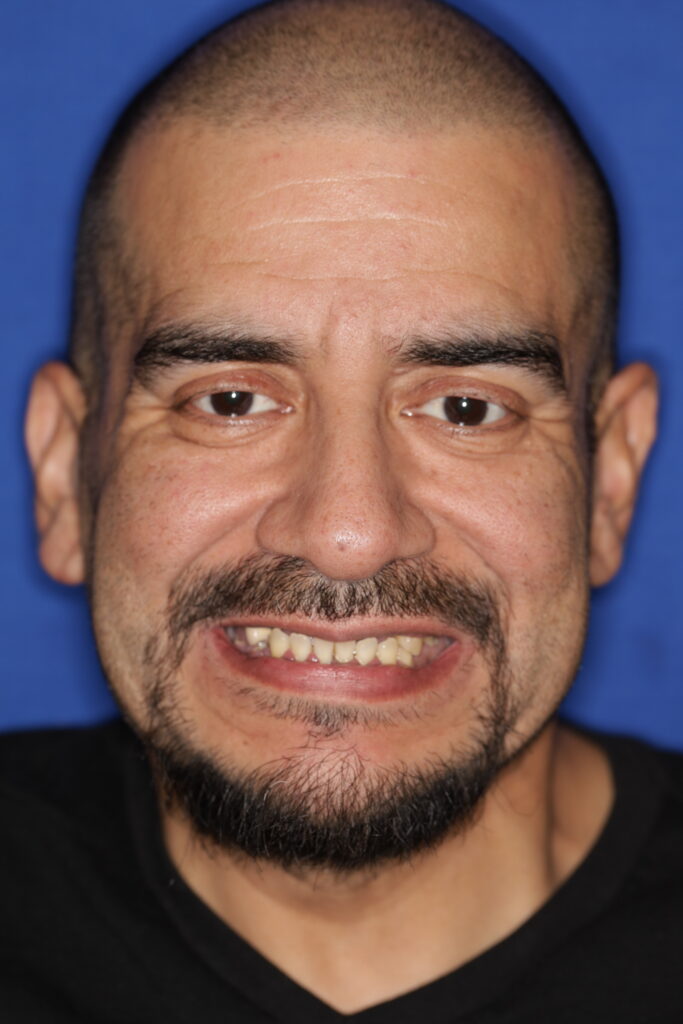
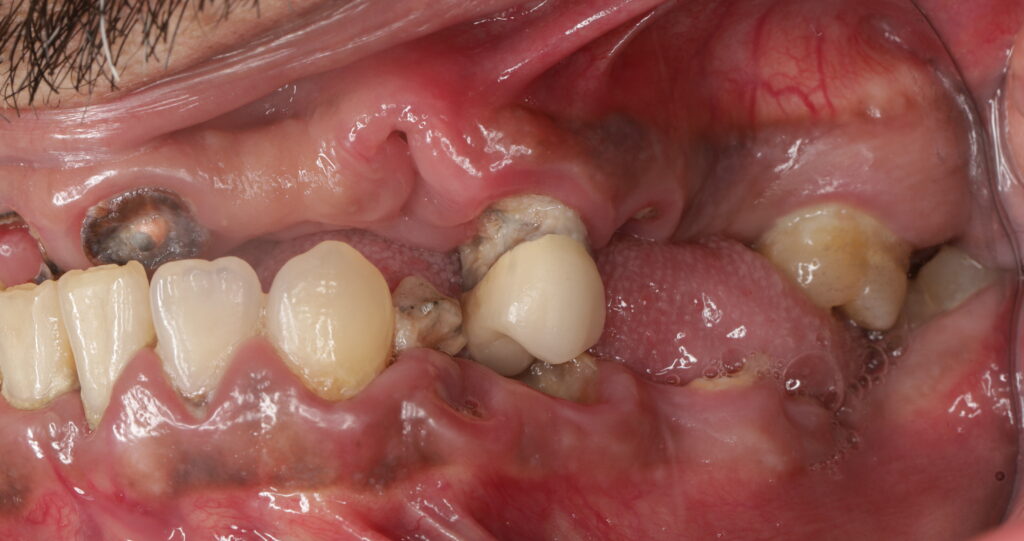
When this patient came in, his teeth were in very bad shape. Multiple infections, broken teeth, tooth loss, and cavities had taken over. Some teeth had broken all the way to the nerve, causing severe pain.
His bite had collapsed — what we call loss of vertical dimension (the distance between the tip of your nose and chin). When that space shrinks, it can affect not only function, but also makes the face look older.
During the initial exam, I found that most of his lower teeth could be saved, except for the lower right molars. My goal was to preserve what was healthy and replace only what we had to. That meant a small dental implant bridge on the bottom and a full replacement on the top.






Planning the New Smile
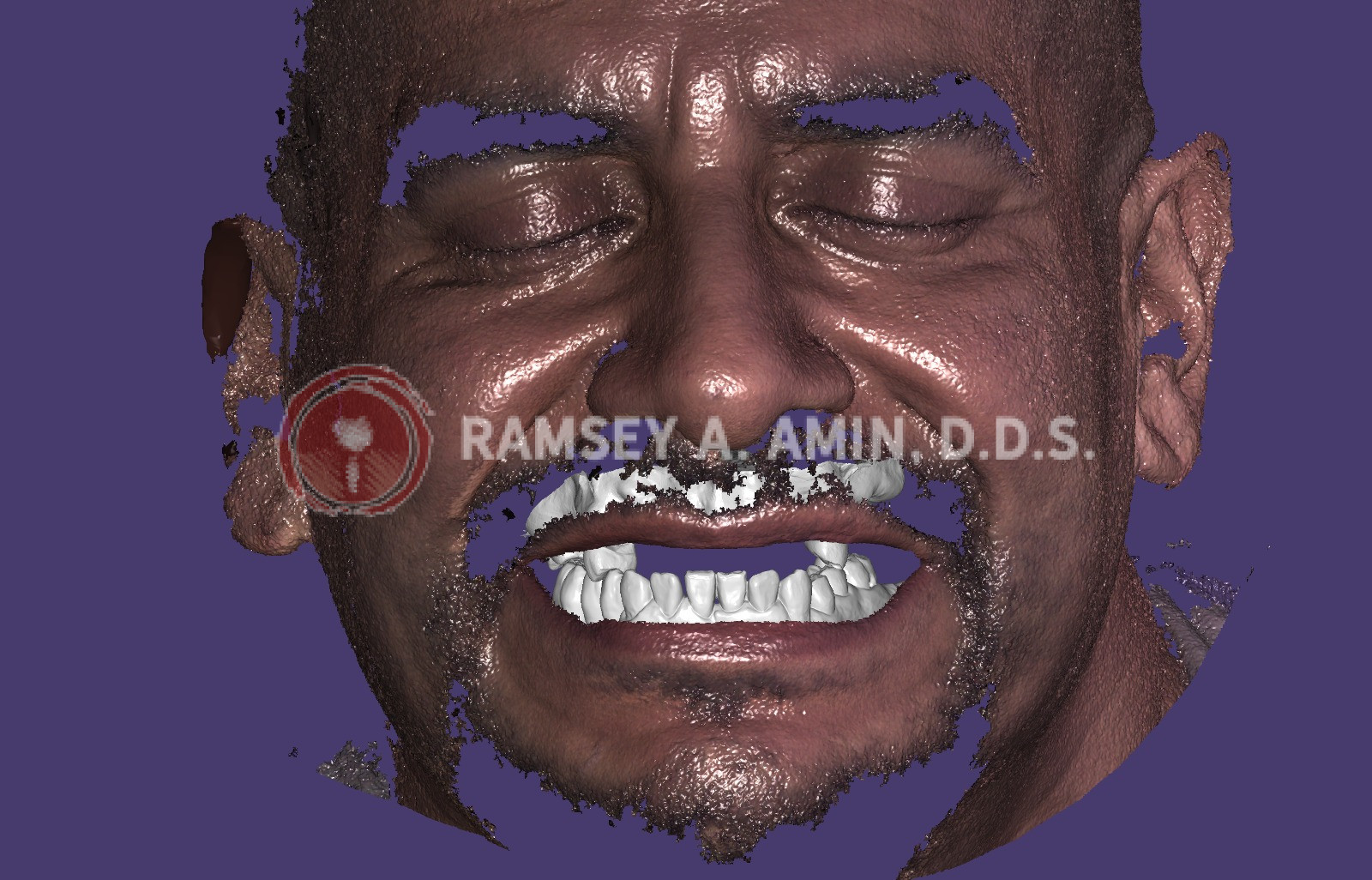
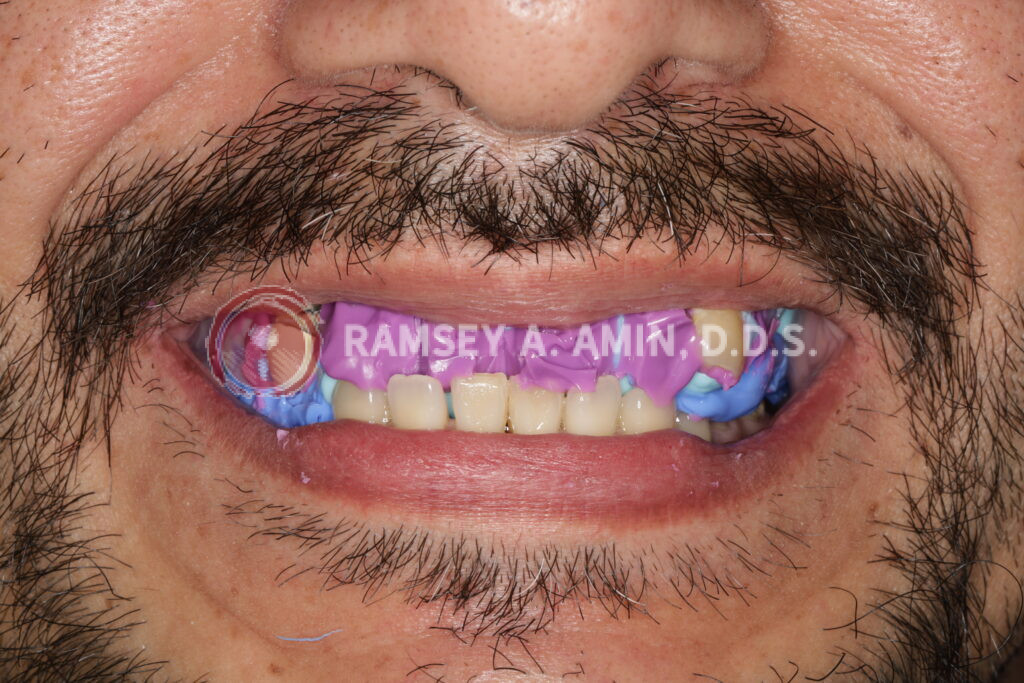
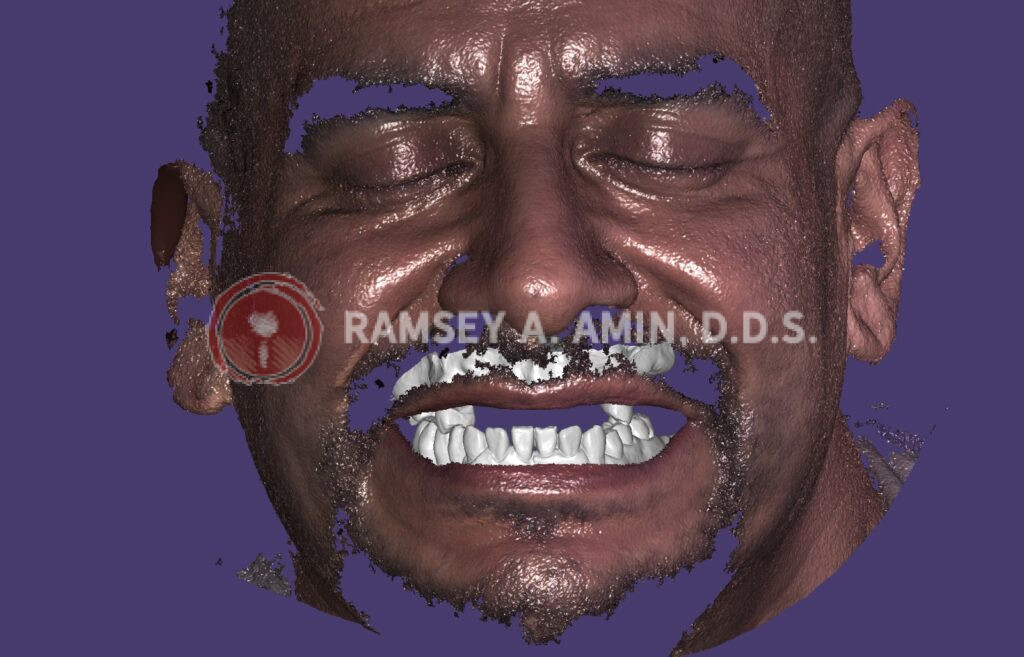
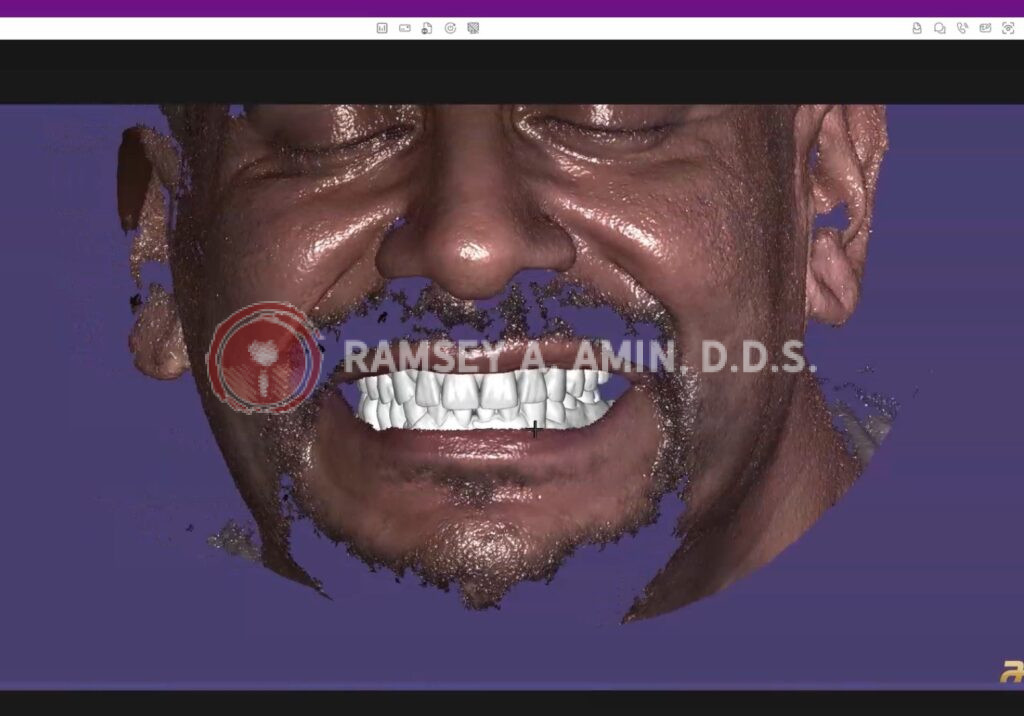
Before any surgery, I do a detailed planning stage. In this case, I used a custom purple smile analyzer that I made with special putty. This was combined with digital facial scanning technology to simulate his future smile — size, shape, and proportions.
This “prototype” is finished before treatment day so that I know exactly what the final result will look like. There are no surprises.

The Surgery Day
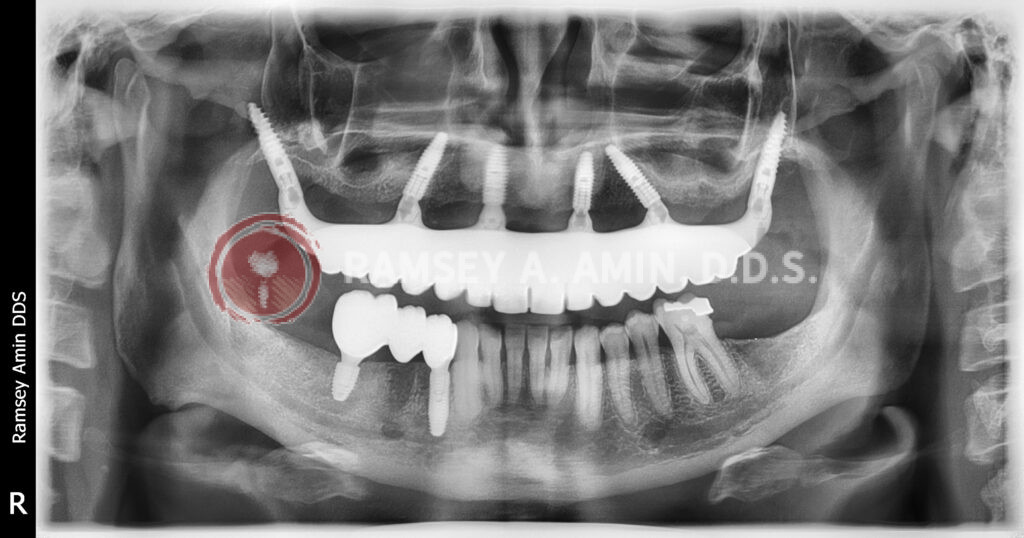
Under safe IV sedation, my patient slept comfortably through the entire procedure. I removed the bad teeth and carefully placed all the dental implants — even some pterygoid implants in the upper jaw for extra stability.
Because he’s young, I preferred to use six implants on the upper instead of just four. Upper implants experience more stress over time, and the extra support goes a long way.
On the lower jaw, I removed the damaged teeth and placed implants into the sockets immediately — all in one visit.
Even a deep cleaning was done on the teeth to be saved!
After placement, I used dissolvable sutures and injected EXPAREL® to help with post-op pain. I also used a combination of anti-inflammatory medication, a mild steroid, and non-OTC Arnica Montana to reduce swelling. Most of my patients, including him, need nothing stronger than ibuprofen afterward. No heavy pain meds.
The Immediate Transformation
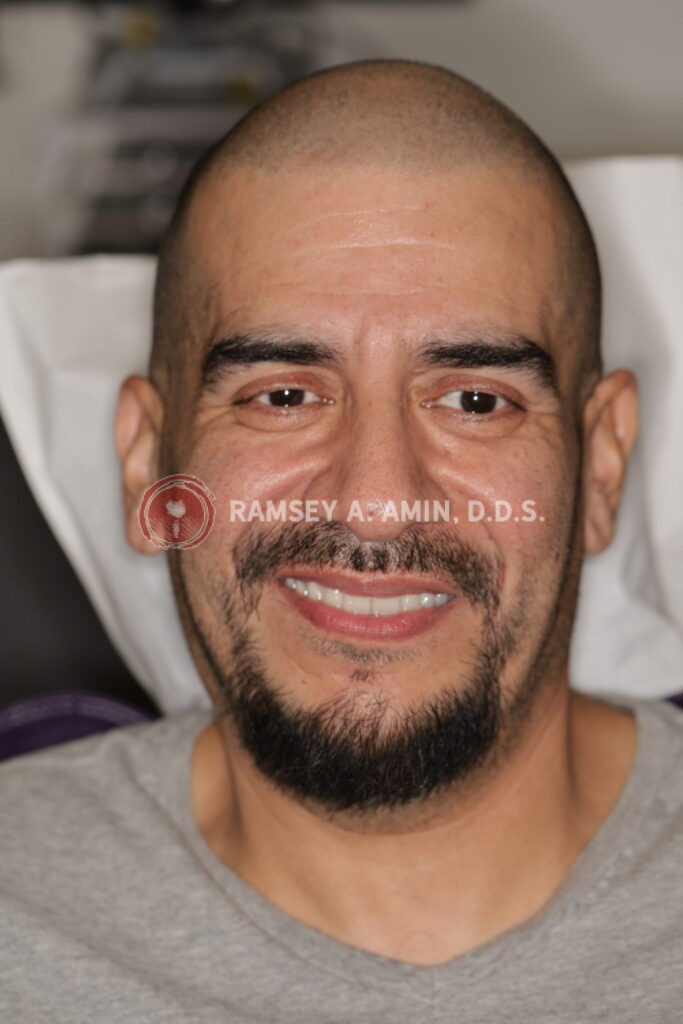
The very next day, he received his temporary healing dental implants, designed and milled by my expert lab team. They were screwed into place in about 30 minutes.
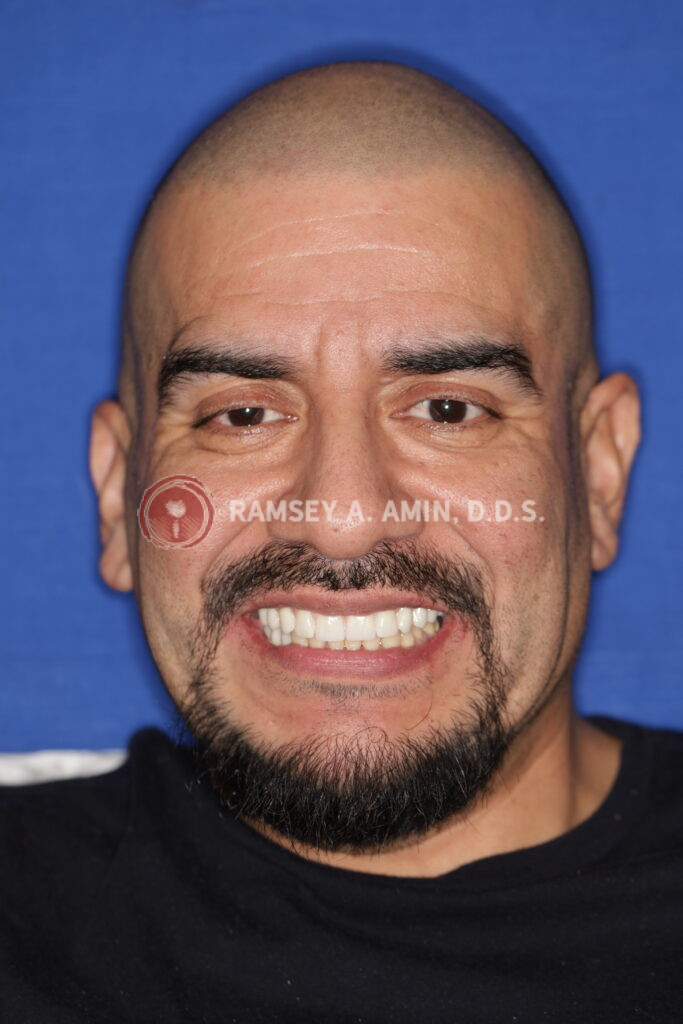
The look on his face said it all. That new smile gave him back more than just teeth — it gave him confidence, health, and energy again.
I always tell my patients, “Implants don’t just give you teeth — they give you your life back.”




Healing and the Final Zirconia Teeth
He healed greatly over four months. During that time, his diet was limited to soft foods — anything you can squish with your fingers. No chewing on pizza or sandwiches for a bit, but it’s a small price to pay for long-term success.
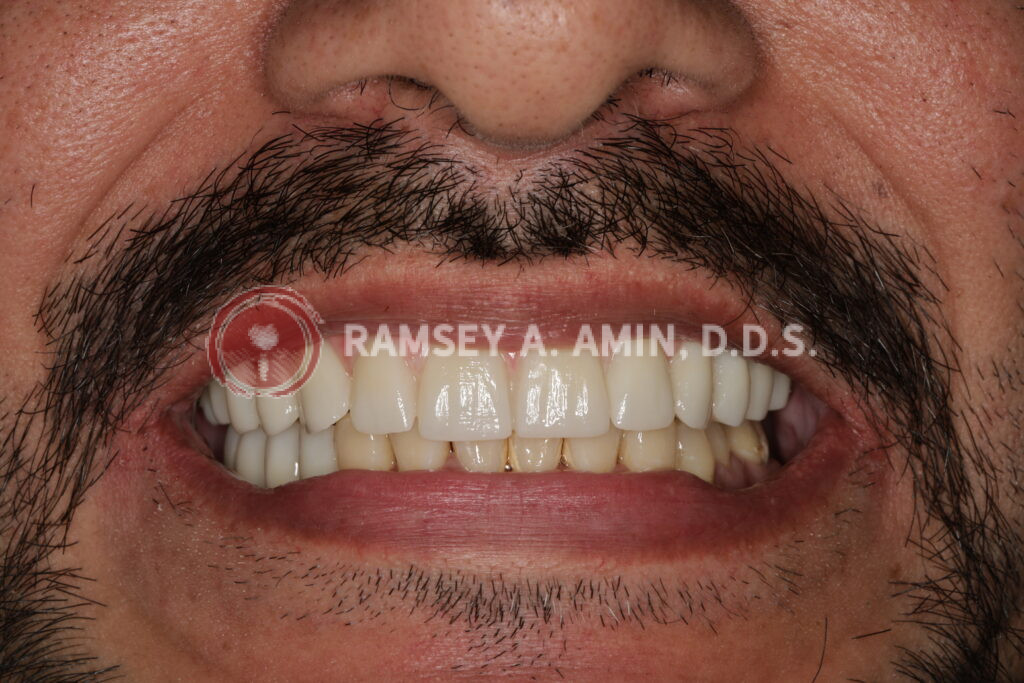
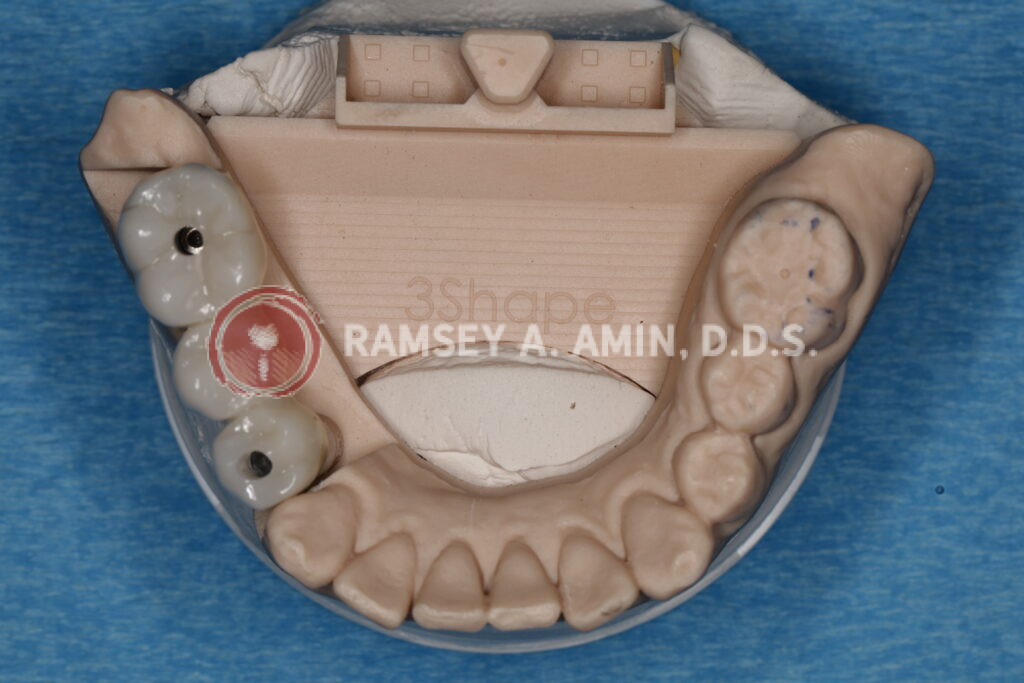
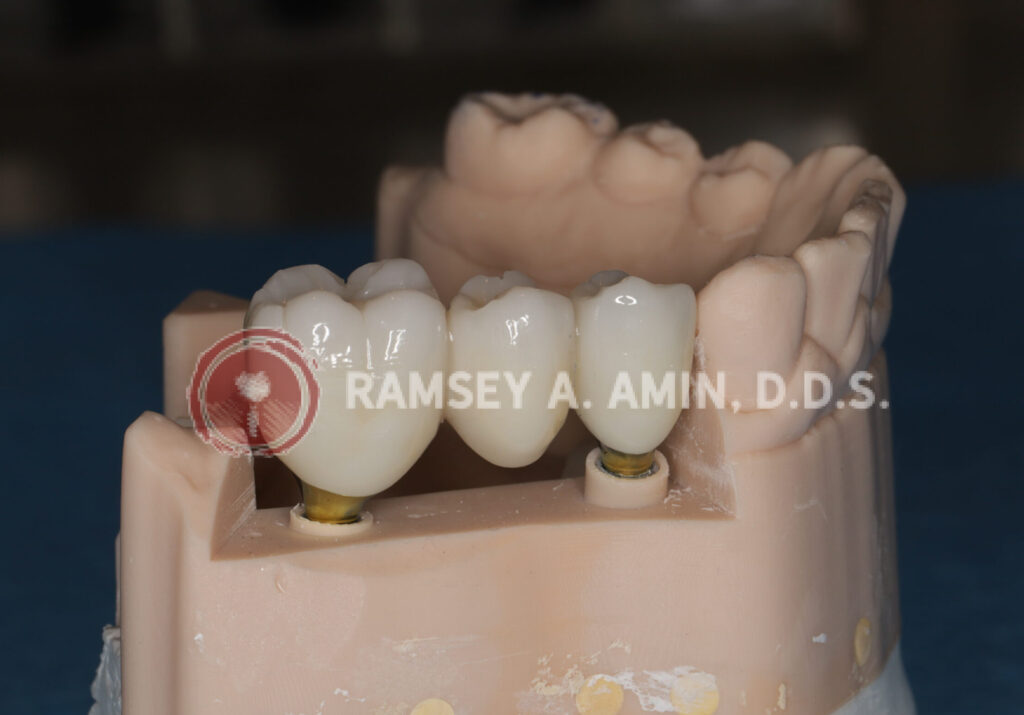
Once healed, I delivered his final zirconia bridge. The final result looked even more natural than his temporaries — teeth with natural spacing, lifelike translucency, and a strong bite. On the bottom, I placed a three-unit implant bridge supported by two implants. It’s a smart and durable design.
Cleaning these implants is simple: a Waterpik is a must.




Premium Design for Long-Term Success After Losing My Teeth
On his upper jaw, I reinforced the bridge with a titanium support bar — hidden inside the zirconia but providing exceptional strength and stability. It’s a premium feature I often recommend when the teeth are designed thinner or for advanced full-arch restorations like FP1.
All infections were completely removed, and I bone grafted the sites using his own bone and regenerative materials. The bone was healthy, the gums healed perfectly, and his framework looked exactly how I had planned from day one.
The Takeaway
This is the process that most of my full-arch implant patients go through. It’s smooth, efficient, and predictable — no guessing, no shortcuts.
Unfortunately, I see a lot of patients in their 40’s and 50’s who come in after failed implants placed elsewhere. Sadly, about 35% of my cases today involve redoing or repairing others’ work.
My advice? Do it right the first time. Experience matters, especially when it’s something you rely on every single day.


I’ve added some images of his case and the digital facial planning workup so you can see the process step by step.
Afraid that losing my teeth might become part of your reality? Don’t lose hope.
If you’re in your 40s or 50s and experiencing tooth loss, just know that there’s a proven way to restore your smile — and your confidence — for life.
Feel free to ask any questions in the comments below—I actually read them and do my best to respond.
Ramsey A. Amin, D.D.S.
Diplomate, American Board of Oral Implantology / Implant Dentistry
Honored Fellow, American Academy of Implant Dentistry
Dr. Amin, Thank you for posting such informative blogs and for giving quality feedback.
Please let me know if you have suggestions on my situation. The below work was done by different doctors at various locations I had lived in the Eastern U.S.; I’m in my early 60s.
Using international numbering, #4 had RCT with porcelain over metal crown in early 1990s and #5 had a similar crown at that time. In 2013, I had #2 extracted due to damage from an impacted #1, that was extracted at the same time. At the time, it was noted that #2 penetrated my sinus cavity such that the root hole was closed to seal this opening. The #2 penetration had caused tooth pain when I had sinusitis. And, I have had chronic sinus congestion since my teens, which is not allergy related (per allergist) and shifts sides based on sleeping position. Also, #16 and #17 were extracted in 1990s.
A recent digital 3D scan shows that there is an abscess above both #4 & #5 with bone loss (no pain), and, separately, #3 has no bone support (no visible infection, gum intact), which I don’t recall from the #2 extraction, but I can feel the difference in support. The examining Endodontist proposed a few options that follow, with his paraphrased concerns and comments noted on each, and I’m trying to get additional information to make a fully informed decision. The options proposed are:
Option 1) extract #3, retreat (RCT) #4, and RCT #5. Concern with this option is lack of teeth above #30 & #31 (#32 is still well receded) and migration upwards. Without bone, an implant for #3 is not practical.
Option 2) postpone #3, retreat (RCT) #4, and RCT #5. Concern with this option is #3 has a less than 50% survival prognosis, which means we’re only postponing the inevitable extraction and chancing possible reinfection of the area.
Option 3) extract #3 and #4, and RCT #5, with consideration of a partial denture for #2-4. Concern is loss of #4 and eventually #5 given need to retreat #4. Note: There is a bridge across #13-15 from loss of #14 in late 1980s.
Option 4) endodontic apicoectomy for the abscess. Concern is invasive process and poor prognosis of the effectiveness, which just postpones one of the above options as it likely won’t improve #3’s situation.
The big question to me is whether a particular option has more benefit in quality of life than the others, or if there is another option that we’re all missing? I’d rather not lose any more teeth (impact to chewing and #30-31) in that area, which is making selecting the Endodontist’s choice of option 1 difficult. Also, I am concerned that there is an underlying issue that will eventually progress farther forward. Although nothing is obvious, the bone loss progression is bothering me.
Of course without seeing you there is no way to truly advise you. I would avoid option 4 though. You may spend a ton of money trying to save teeth that ‘may’ be just better off extracting 3, 4 and 5 and having implants instead. This is to be CAREFULLY explored before making this decision. I am doing this exact combo on Tuesday morning. The bone can easily be added to #3 ext site and usually at the same time of the extraction! I often do all of this in a SINGLE procedure. Find the right DDS first! Good luck!
Thank you for the feedback! This has helped inform me on the options.
This is an incredible case. It really shows how full-arch implants can completely restore both function and confidence, even in complex situations.
I would like someone to get back to me thank you
Hi –there was no question or text to be able to reply. Sorry! Dr. Amin