
(updated February 2025)
This patient has severe bone loss of the lower front teeth area. He wants implants, but was told by numerous dentists it could not be done.
A huge part of my practice in Burbank, California is devoted to treating these very difficult dental implant cases where huge bone grafts may be needed. I was confident I could treat him with a long-lasting bone grafting and implants result.

Let’s review this dental implant and bone grafting case
There are two options with bone loss this severe in a relatively small area of the mouth.
- Option 1: Rebuild the bone back through grafting to its original height and width.
- Option 2: Use the existing bone and do not rebuild the bone through grafting procedures. (This is a similar concept like zygomatic implants for upper full reconstruction)
Both options have their merits and I perform both procedures. You must carefully choose with the judgment of your implants dentist which is better.
Ideally, I would like to graft the bone back for this patient so that his teeth could look, feel and function just like the original. The reality is that building vertical height and maintaining it over time is quite difficult for any expert surgeon, even as of 2023. I’m not saying that bone grafting vertical height cannot be done, it just is extremely difficult in this particular situation.

In his situation he’s missing bone on the tongue side almost to “floor of the mouth.” The floor is where the tongue rests.
When you’re missing the “inside” bone on the tongue or on the upper palate, that bone does not rebuild very well (even with BMP and L-PRF) . The outer bone grows a lot easier on the cheek side.
Particularly the muscles of the tongue want to pull bone downward even when I do complex reconstructions with titanium mesh or block bone grafts.
Option 2 was my choice for this particular implants case
So even though I can rebuild it, I chose option two because the stability of the rebuilt bone over time will likely not last due to the muscles of the tongue and the muscles of the chin and lips pulling it back down.
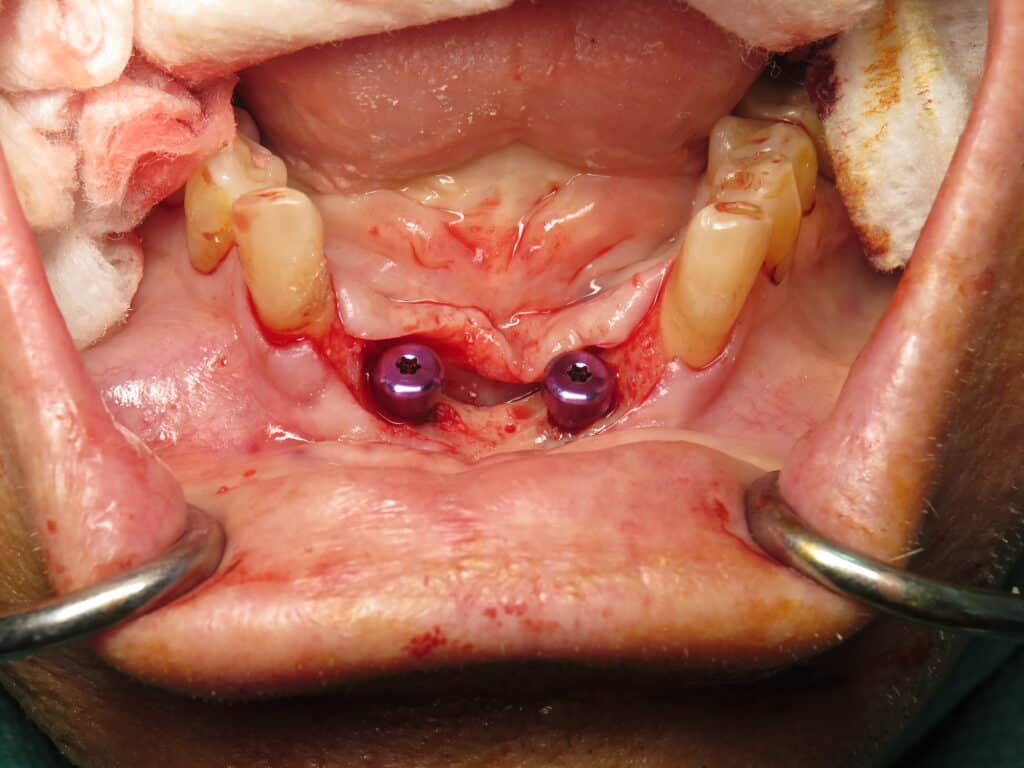
The goal here was to use his existing bone, but to augment the gums.
I did a gum graft from his palate to strengthen the gum tissue from the tension of the lip and tongue muscles. This creates a nice attached thick gum that won’t move around once the implants are in and it creates a seal.


Under intravenous sedation, I placed two very strong titanium alloy grade 23 implants to precise positions after the gum graft was allowed to heal for about six weeks. During this time he continued to use his removable plate that he came with.
After integration was confirmed, I used my digital Trios scanner to take digital impressions.


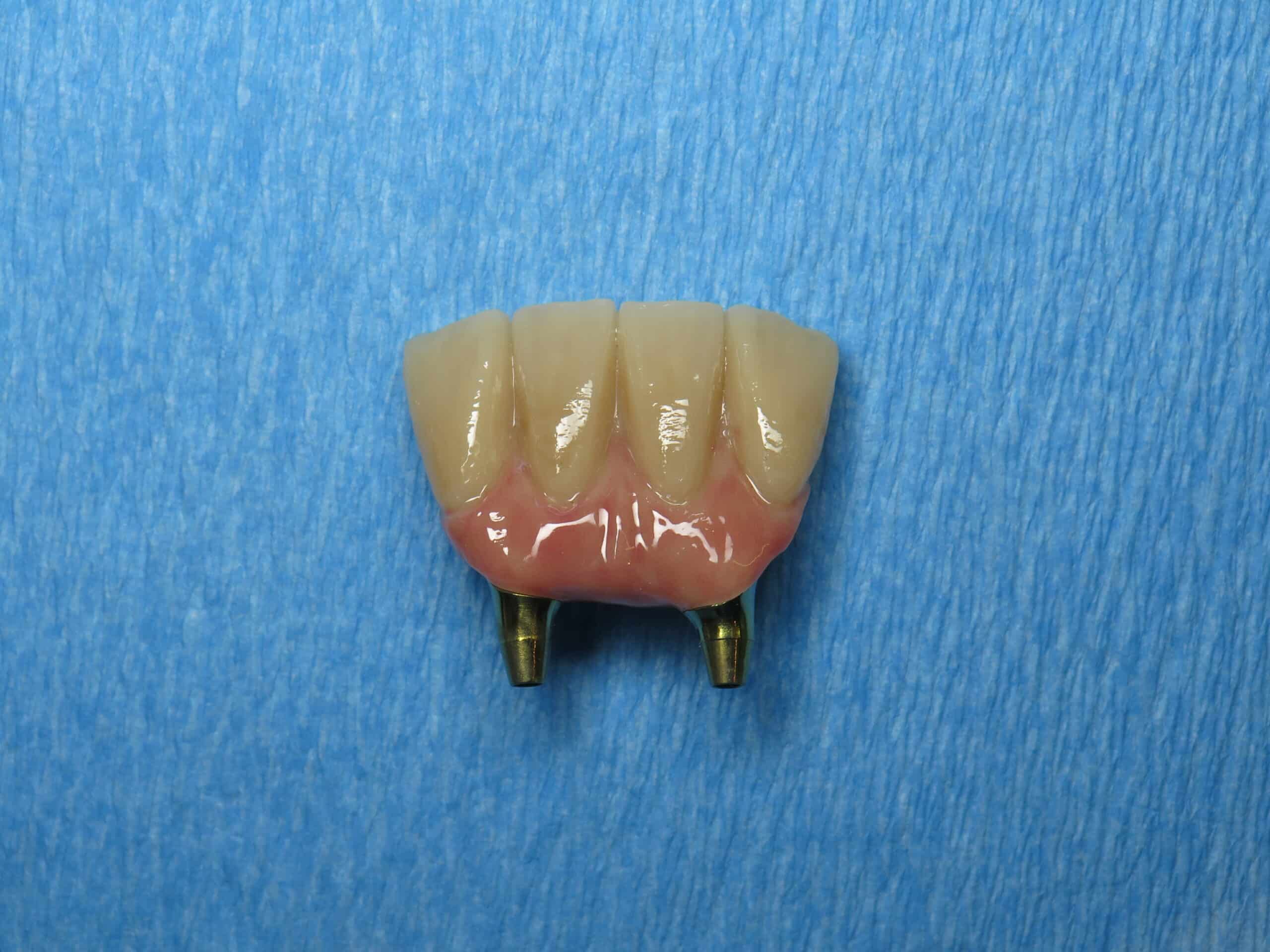
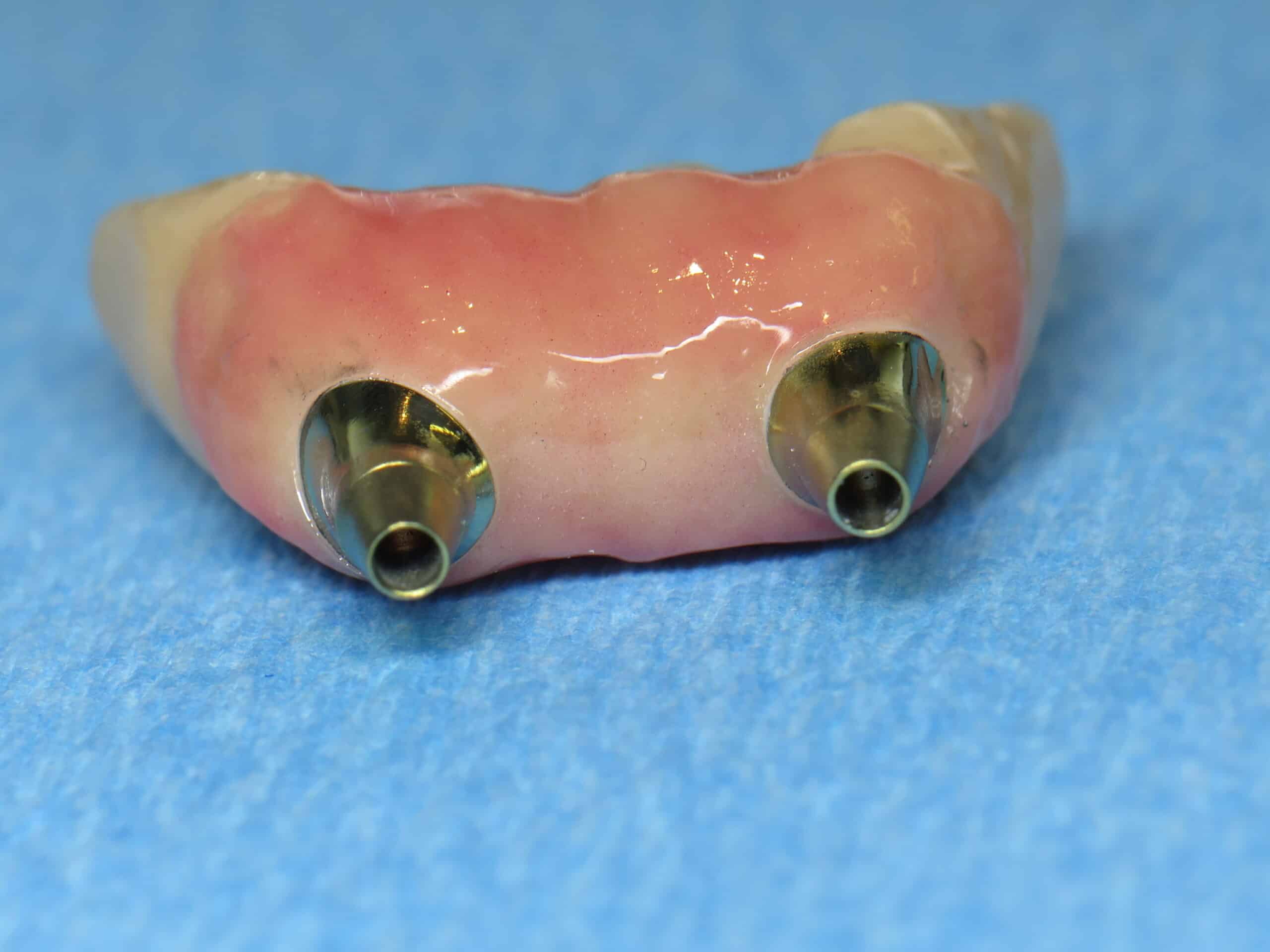


The case was designed in tandem with my expert lab technician. The goal was to have a convex shape like I would for any full arch replacement along with gum colored ceramics. The teeth making process is complex and needs to be done well to avoid problems!
It was imperative that the patient is able to floss underneath and use a WaterPik with the U-turn bend.
These pictures were taken a year after placement and he is doing great.
The result?
So option two was used because the bone for the implants would be stable since it is his own native bone (not regrown). Of course you want “no pink,” but having the implants lose rebuilt bone in just 1-3 years is unacceptable to me. Keep in mind that 90% of cases are not like this!
If you need more information about bone grafts, please visit my page dedicated to general information about bone grafts.
Please comment below and thank you for reading! I hope this helps!
- Ramsey Amin, D.D.S. of Burbank Dental Implants
- Diplomate of the American Board of Oral Implantology /Implant Dentistry
- Fellow-American Academy of Implant Dentistry
- 818-846-3203
Dr Ramsay, I have severe periodontal disease in my lower front teeth with around 2/3 bone loss. I am 36 and have never smoked… After comprehensive scale and root planning to preserve lower teeth maybe some stinting what options are available to me?
A bridge on two implants for 4 lower front teeth is generally enough ! Here are two examples!
https://burbankdentalimplants.com/immediate-implant-bridge-lower-jaw-front-teeth/
https://burbankdentalimplants.com/lower-front-teeth-dental-implants-with-gum-graft-and-immediate-temporaries/
Dr. Ramsey Amin
70 year old with osteoporosis but do not take any osteoporosis medicines. Tooth #3 was extracted two weeks ago by oral surgeon due to infection without socket bone graft.
Tooth #3 had history of abscess, root canal, crown lengthening 14 years ago.
Should I do the allograft socket bone graft now three weeks post extraction so there is no bone loss?
How long does the socket bone graft last?
I don’t know how soon I would do the sinus lift and implant.
Thank you so much for doing this awesome blog.
Thank you for your kind words. The best time to have done the socket graft would have been to be at the time of extraction.
The graft will only last for maybe one to three years and then begin to shrink if you don’t place the implant. A more advanced way to do all of this would be to do what I call early placement… That means I don’t do the graft and go ahead and place the implant and graft around it.
This is incredible !!
This is how bad my mouth is. I don’t know where to start or what to do. It’s starting to affect my mental health.
Hello Dr. Ramsey,
I have a severe bite that slides to the left when I close my mouth. Along with clenching and grinding.
I have 3 dental implants and in process of a redo implant on top front tooth due to it was to large and causing immense pain. My teeth- crowns are worn from grinding. Guards do not help as I grind them and they seem to cause pressure on my teeth. When I grind and slide it is causing severe pain as I am hitting and locking into my teeth.
Causing root canals and recent bone spur. I am 63 and live in turmoil. What would be an option for me so I do not slide and clench into my teeth. I have tmj and tinnitus. I was prescribed a low dose of Valium to help with clenching but it is the cross slide that is really the culprit to constant pain in my teeth, gums and jaw.
I appreciate any feedback.
This page discusses the use of Botox® for managing issues related to teeth grinding, jaw clenching, and dental implants. It explains that Botox® can be important for dental implant patients who have issues with grinding or clenching, as these activities can exert high biting forces on the implants, potentially leading to failure. The article describes how Botox® is used to temporarily decrease the strength of the biting muscles, thereby reducing the risk of implant failure. It also addresses concerns about Botox® affecting facial appearance, assuring that its use in this context does not alter facial looks but rather aims to reduce bite force for therapeutic reasons.
Dr. Amin- I am caretaker for elderly relative who recently was diagnosed with osteoporosis and now taking meds for it. She has had lower dental implants ( due to accident) for at least 5 years- it replaces about 4 teeth. She is concerned about the meds eroding the bone that serves as anchors for the implants–as she had localized gum grafting to the area prior to the implant. Would there be anything that she or I should ask her periodontist at next visit? Thank you.
Just take some updated x-rays. I would highly suggest that she is using a WaterPik on a daily basis since this is an implant bridge. Most people cannot clean as well as they think they are. The proper order would be to brush first, floss using floss threaders and then WaterPik last.
Here is an article on how to clean dental implants
hi am in NEW ZEALAND in process to get quad zgoma inplants person to make teeth said need front part bone removed,re build out sides upper lip i will get facial implants as your bridges look amazing, do you have site i can get them to view .we are behind here,ive upper denture hate it long time caused depression list goes on, am under oral surg thank you
This article has a link within the quad zygo article for lip support. Check it out.
https://burbankdentalimplants.com/quad-zygomatic-dental-implants-to-replace-dentures-without-bone/